Jaundice
Overview
Also known as icterus, jaundice describes the yellowish pigmentation of the skin and sclera due to high serum bilirubin levels as a result of interference in the normal metabolism of bilirubin.
Jaundice becomes apparent when the serum bilirubin levels are over 35 μmol/L. The presence of jaundice can suggest problems with the liver, biliary tract, or blood (e.g. haemolytic anaemia).
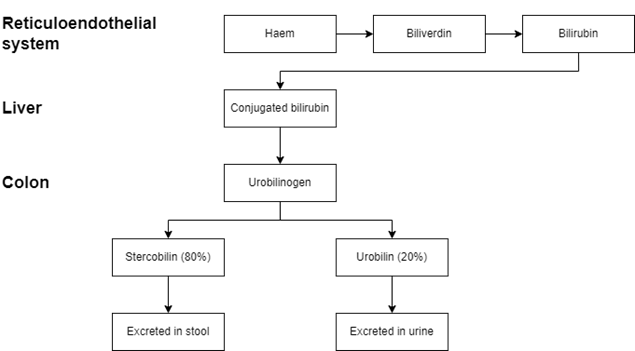
Bilirubin metabolism and excretion: a summary
In the reticuloendothelial cells, haem (found in haemoglobin) is converted to biliverdin and then converted to bilirubin. In the liver, bilirubin is converted into conjugated (direct) bilirubin, making it soluble and easier to excrete. Some bilirubin can escape the process and remain as unconjugated (indirect) bilirubin, which is insoluble.
Conjugated bilirubin is excreted into the duodenum in bile. Once it reaches the colon, bacteria deconjugate the bilirubin and convert it into urobilinogen. 80% of this urobilinogen is eventually converted into stercobilin, giving faeces their colour. The remaining 20% is reabsorbed into the blood, which is processed in the liver for bile production. Some of the remaining 20% reaches the kidneys where it is oxidised into urobilin and excreted in the urine.
Pre-hepatic (haemolytic) jaundice
This form of jaundice is most commonly caused by a pathologically increased rate of red blood cell haemolysis. Haemolysis releases high levels of unconjugated bilirubin, which overwhelms the liver, leading to the deposition of unconjugated bilirubin in tissues. Causes may be:
- Hereditary and acquired causes of haemolytic anaemia
- Gilbert’s syndrome – impaired bilirubin conjugation
Since the bilirubin is unconjugated, it cannot be excreted into the intestines, leading to dark stools and urine that darkens when left to stand, as urobilin forms as more time progresses.
Hepatic (hepatocellular) jaundice
This form of jaundice is due to damage to the hepatocytes, leading to an inability of the liver to conjugate bilirubin. Both unconjugated and conjugated bilirubin levels increase. Causes may be anything that can cause direct liver damage:
- Toxic:
- Alcohol
- Paracetamol
- Infectious:
- Hepatitis A, B, C, D, and E
- HIV infection
- Plasmodium falciparum malaria
- Entamoeba haemolytica
- Leptospirosis
- Autoimmune:
- Other:
Post-hepatic (cholestatic) jaundice
This form of jaundice is due to a blockage of the bile ducts that transport bile and conjugated bilirubin out of the liver. The liver can conjugate the bilirubin, but cannot excrete it, leading to high amounts of conjugated bilirubin. Causes may be:
- Gallstones (choledocholithiasis)
- Iatrogenic injury
- Ascending cholangitis
- Pancreatic cancer
- Cholangiocarcinoma
- Biliary atresia
- Primary biliary cirrhosis
- Cystic fibrosis
- Lymphoma
- Pregnancy
Since less conjugated bilirubin is excreted into the intestinal tract, less urobilinogen is produced. This results in less stercobilin, leading to pale stools. Although there is less urobilin (due to the lack of urobilinogen), the excess conjugated bilirubin is excreted in the urine, giving dark urine.
Initial investigations
The investigations for a patient with jaundice are the following. Interpretation of these results is under the ‘Typical findings’ heading below:
- Liver function tests (LFTs)
- Conjugated and unconjugated bilirubin levels
Other investigations
- Full blood count (FBC) – for haemolysis
- Hepatitis serology
- Ferritin – for haemochromatosis
- Autoantibodies (e.g. serum antinuclear antibodies (ANA) or anti-smooth muscle antibodies) for autoimmune causes
- Alpha-1-antitrypsin (A1AT) levels – for A1AT deficiency
- Abdominal ultrasound – useful for gallstones or other causes of obstruction
- Magnetic resonance cholangiopancreatography (MRCP) – useful for gallbladder pathology
Typical findings
A summary of typical investigation findings for jaundice is as follows. It is important to remember there may be overlap between different diseases, making the diagnosis more difficult.
| Measure | Pre-hepatic | Hepatic jaundice | Post-hepatic |
| Total serum bilirubin | Normal or elevated | Elevated | Elevated |
| Conjugated bilirubin | Normal | Elevated | Elevated |
| Unconjugated bilirubin | Normal or elevated | Elevated | Normal |
| Urobilinogen | Normal or elevated | Decreased | Decreased |
| ALT and AST | Normal | Highly elevated | Elevated |
| ALP | Normal | Elevated | Highly elevated |
| Urinary conjugated bilirubin | Absent | Present | Present |
| Urine colour | Normal | Dark | Dark |
| Stool colour | Normal | Normal or slightly pale | Pale |
Signs Relating to the Biliary Tree
Boas’ sign
Boas’ sign describes hyperaesthesia in the right lower scapular region or right upper quadrant of the abdomen. It is associated with acute cholecystitis.
Courvoisier’s law
Courvoisier’s law states that a painless palpable mass in the right upper quadrant along with jaundice is unlikely to be due to gallstones. This sign suggests the presence of pancreatic cancer or cholangiocarcinoma.
Charcot’s triad
Charcot’s triad describes jaundice, fever, and right upper quadrant pain, which suggest the presence of acute cholangitis.
Reynold’s pentad
Reynold’s pentad describes Charcot’s triad (jaundice, fever, and right upper quadrant pain), along with shock (hypotension with or without tachycardia), and an altered mental status. It suggests serious acute cholangitis.
Murphy’s sign
Murphy’s sign describes the arrest of inspiration on palpation of the right upper quadrant. It is tested by asking the patient to breathe out, palpating the right upper quadrant, and asking the patient to breathe in. During inspiration, the abdominal organs move down as the lungs expand and the diaphragm moves down. As the gallbladder moves down and comes into contact with the examiner’s hand, the patient stops breathing in due to pain.
Signs Relating to Abdominal Pain
Abdominal guarding
Abdominal guarding describes the voluntary contraction of abdominal wall muscles in anticipation of pain when the abdomen is palpated to ‘guard’ the underlying inflamed tissue.
Abdominal rigidity
Abdominal rigidity differs from guarding as it describes the involuntary increased tension of abdominal muscles due to underlying inflammation. Rigidity tends to occur over the inflamed area, whereas guarding tends to be generalised over the entire abdomen. Abdominal rigidity suggests peritoneal inflammation.
Rebound tenderness
Rebound tenderness describes pain upon removal of pressure to the abdomen. It suggests the presence of parietal peritoneum inflammation due to stretching.
Rovsing’s sign
Rovsing’s sign describes pain felt in the right lower quadrant when palpating the left lower quadrant. It is associated with appendicitis. Abdominal viscera pain nerves do not localise well and elicit generalised pain. Once the inflammation irritates the peritoneum, the pain becomes localised. Palpation of the left lower quadrant stretches the peritoneum, eliciting pain on the right side when inflamed.
Signs Relating to Abdominal Masses
Hepatomegaly
Hepatomegaly describes an enlarged liver and may occur due to infection, malignancy, cirrhosis, or right heart failure.
Splenomegaly
Splenomegaly describes an enlarged spleen which can result from infection (such as infectious mononucleosis), portal hypertension (e.g. secondary to cirrhosis), and haematological disorders including myeloproliferative disorders, malignancy, and haemoglobinopathy.
Hepatosplenomegaly
Hepatosplenomegaly describes the enlargement of both the liver and spleen. Its cases include, but are not restricted to, liver cirrhosis, right-sided heart failure, infection, and haematological disorders including myeloproliferative disorders, malignancy, and haemoglobinopathy.
Sister Mary Joseph nodule
The Sister Mary Joseph nodule describes a periumbilical nodule. Its presence may suggest the presence of gastrointestinal malignancy, including gastric cancer and pancreatic cancer.
Virchow’s nodes
The left supraclavicular lymph nodes are known as Virchow’s nodes. If a palpable mass is felt in this region, it may suggest gastric cancer metastasis, as this is one of the first sites it metastasises to.
Signs Relating to Abdominal Distention
Ascites
See Ascites for more information.
Shifting dullness
Shifting dullness is a sign that looks for the presence of ascites. It is done with the patient initially lying flat and percussing the midline of the abdomen. This should give a resonant sound due to the fluid settling to the bottom and gas being present. Percussion then moves away from the examiner until it becomes dull, suggesting the presence of fluid. The examiner’s finger is left at the first point of dullness and the patient rolls onto the other side. Around 10-30 seconds later, this point is percussed again back to the centre. If this point is now resonant, ascites is likely to be present and shift due to gravity.
Other Abdominal Signs
Cullen’s sign
Cullen’s sign describes periumbilical discolouration due to oedema and bruising. It occurs due to intra-abdominal bleeding and is seen in acute pancreatitis and abdominal trauma.
Grey Turner’s sign
Grey Turner’s sign describes flank discolouration due to bruising secondary to retroperitoneal haemorrhage. It is associated with acute pancreatitis.