Overview
Also known as icterus, jaundice describes the yellowish pigmentation of the skin and sclera due to high serum bilirubin levels as a result of interference in the normal metabolism of bilirubin. Jaundice becomes apparent when the serum bilirubin levels are over 35 μmol/L.
The presence of jaundice can suggest problems with the liver, biliary tract, or blood (e.g. haemolytic anaemia).
Overlapping types
The overall types of jaundice are discussed below. It is important to note that they can overlap as many of their causes can cause damage to surrounding tissues.
For example, cholangiocarcinoma may initially present with post-hepatic jaundice with cholestatic liver function tests, but if the tumour invades the liver, pre-hepatic jaundice can arise and hepatitic liver function tests can appear.
Types of Jaundice
Pre-hepatic
Pre-hepatic (haemolytic) jaundice describes elevated unconjugated bilirubin before the liver cells conjugate bilirubin. It occurs due to haemolysis overwhelming the liver’s capacity to conjugate bilirubin or inadequate bilirubin conjugation (Gilbert’s syndrome).
Liver disease can cause elevations in unconjugated bilirubin, but this is initially mixed with conjugated bilirubin until later stages when the hepatocytes can no longer conjugate bilirubin.
Hepatic (hepatocellular) jaundice
Hepatic (hepatocellular) jaundice occurs due to damage to the liver cells, resulting in a reduction in their ability to conjugate bilirubin. Its causes include direct liver damage such as viral hepatitis, autoimmune diseases, drugs and toxins (e.g. alcohol and paracetamol), and metabolic disorders (e.g. Wilson’s disease).
Liver disease can cause elevations in unconjugated bilirubin, but this is initially mixed with conjugated bilirubin until later stages when the hepatocytes can no longer conjugate bilirubin.
Post-hepatic (cholestatic) jaundice
Post-hepatic (or obstructive/cholestatic) jaundice occurs due to the blockage of the bile duct that transports bile and conjugated bilirubin out of the liver.
The liver can conjugate bilirubin, but it cannot be transported effectively and accumulates in the blood, resulting in elevated conjugated bilirubin.
Causes include gallstones in the common bile duct, pancreatic cancer, cholangiocarcinoma, biliary strictures and cirrhosis, and pregnancy.
Post-hepatic jaundice cause pale stools and dark urine as less conjugated bilirubin can be excreted in the faeces and more has to be excreted in the urine.
Bilirubin Metabolism and Excretion
Bilirubin metabolism
In the reticuloendothelial cells, haem (found in haemoglobin) is converted to biliverdin and then converted to bilirubin. In the liver, bilirubin is converted into conjugated (direct) bilirubin, making it soluble and easier to excrete. Some bilirubin can escape the process and remain as unconjugated (indirect) bilirubin, which is insoluble.
Bilirubin excretion
Conjugated bilirubin is excreted into the duodenum in bile. Once it reaches the colon, bacteria deconjugate the bilirubin and convert it into urobilinogen. 80% of this urobilinogen is eventually converted into stercobilin, giving faeces their colour. The remaining 20% is reabsorbed into the blood, which is processed in the liver for bile production. Some of the remaining 20% reaches the kidneys where it is oxidised into urobilin and excreted in the urine.
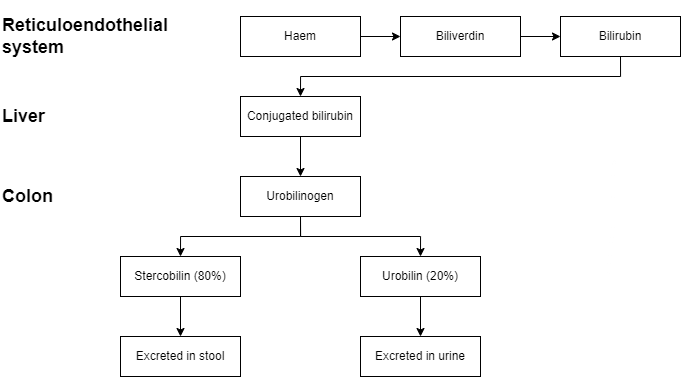
Figure 1: A summary of bilirubin metabolism and excretion
Pre-Hepatic (Haemolytic) Jaundice
Overview
Pre-hepatic (or haemolytic) jaundice is most commonly caused by a pathologically increased rate of red blood cell haemolysis. Haemolysis releases high levels of unconjugated bilirubin, which overwhelms the liver, leading to the deposition of unconjugated bilirubin in tissues.
Causes
Causes may be:
- Hereditary and acquired causes of haemolytic anaemia
- Gilbert’s syndrome – impaired bilirubin conjugation
Since the bilirubin is unconjugated, it cannot be excreted into the intestines, leading to dark stools and urine that darkens when left to stand, as urobilin forms as more time progresses.
Hepatic (Hepatocellular) Jaundice
Overview
Hepatic (or hepatocellular) jaundice is due to damage to the hepatocytes, leading to an inability of the liver to conjugate bilirubin. Both unconjugated and conjugated bilirubin levels increase.
Causes
Causes may be anything that can cause liver damage:
- Toxic:
- Alcohol
- Paracetamol
- Infectious:
- Hepatitis A, B, C, D, and E
- HIV infection
- Plasmodium falciparum malaria
- Entamoeba haemolytica
- Leptospirosis
- Autoimmune:
- Other:
- Non-alcoholic fatty liver disease
- Wilson’s disease
- Hereditary haemochromatosis
- Alpha-1 antitrypsin deficiency
- Hepatocellular carcinoma
- Liver metastases
- Lymphoma
Post-Hepatic (Cholestatic/Obstructive) Jaundice
Overview
Post-hepatic (or cholestatic/obstructive) jaundice is due to a blockage of the bile ducts that transport bile and conjugated bilirubin out of the liver.
The liver can conjugate the bilirubin, but it cannot be transported properly, resulting in its accumulation in the blood. It causes pale stools and dark urine as less conjugated bilirubin can be excreted in the faeces and more has to be excreted in the urine.
Causes may be:
- Gallstones (choledocholithiasis) in the common bile duct
- Iatrogenic injury
- Ascending cholangitis
- Pancreatic cancer
- Cholangiocarcinoma
- Biliary atresia
- Primary biliary cirrhosis
- Cystic fibrosis
- Lymphoma
- Pregnancy
- Mirizzi syndrome
Since less conjugated bilirubin is excreted into the intestinal tract, less urobilinogen is produced. This results in less stercobilin, leading to pale stools. Although there is less urobilin (due to the lack of urobilinogen), the excess conjugated bilirubin is excreted in the urine, giving dark urine.
Initial Investigations
Overview
The investigations for a patient with jaundice are the following. Interpretation of these results is under the ‘Typical findings’ heading below:
- Liver function tests (LFTs)
- Conjugated and unconjugated bilirubin levels
Other investigations
- Full blood count (FBC) and reticulocyte count:
- May show normocytic anaemia and increased reticulocyte count in haemolysis
- Hepatitis serology:
- If viral hepatitis is suspected
- Ferritin and iron studies:
- For haemochromatosis
- Autoantibodies:
- Such as serum antinuclear antibodies (ANA) or anti-smooth muscle antibodies for autoimmune causes
- Alpha-1-antitrypsin (A1AT) levels:
- For A1AT deficiency
- Abdominal ultrasound:
- Useful for gallstones or other causes of obstruction
- Magnetic resonance cholangiopancreatography (MRCP):
- Useful for biliary tree pathology
Typical Findings in Liver Function Tests
Overview
Knowing the origin of other markers alongside bilirubin in liver function tests can help with narrowing down the cause of jaundice. A small summary is as follows:
- Alanine transaminase (ALT):
- Mainly found in the cytoplasm of liver cells, but also found in the kidney, muscles, and heart.
- Elevated levels may suggest liver damage
- Aspartate transaminase (AST):
- Mainly produced in the liver, but is less specific than ALT as it is found in the mitochondria or liver cells and also found in the kidney, muscles, and heart
- Elevated levels may suggest liver damage
- Gamma-glutamyltransferase (GGT):
- Found in hepatocytes and biliary cells and useful when interpreted together with alkaline phosphatase ALP
- Elevated ALP and elevated GGT suggests cholestasis
- Elevated ALP and normal GGT suggests bone disease
- Elevated GGT is associated with alcohol consumption
- Alkaline phosphatase (ALP):
- Found in biliary cells and bones and useful when interpreted together with GGT
- Elevated ALP and elevated GGT suggests cholestasis
- Elevated ALP and normal GGT suggests bone disease
- Albumin:
- Tests liver synthetic function
- Sensitive as it is primarily made in the liver, but not specific as other disorders can cause reduced serum albumin
- May be decreased in chronic liver disease but can also be decreased in nephrotic syndrome as it is lost in the urine
Add these to tooltips and conjugated vs. unconjugated LFTs
Typical findings
A summary of typical investigation findings for jaundice is as follows. It is important to remember there may be overlap between different diseases, making the diagnosis more difficult.
For example, cholangiocarcinoma may initially present with post-hepatic jaundice with cholestatic liver function tests, but if the tumour invades the liver, pre-hepatic jaundice can arise and hepatitic liver function tests can appear.
| Measure | Pre-hepatic | Hepatic jaundice | Post-hepatic |
| Total serum bilirubin | Normal or elevated | Elevated | Elevated |
| Conjugated bilirubin | Normal | Elevated | Elevated |
| Unconjugated bilirubin | Normal or elevated | Elevated | Normal |
| Urobilinogen | Normal or elevated | Decreased | Decreased |
| ALT and AST | Normal | Highly elevated | Elevated |
| ALP | Normal | Elevated | Highly elevated |
| Urinary conjugated bilirubin | Absent | Present | Present |
| Urine colour | Normal | Dark | Dark |
| Stool colour | Normal | Normal or slightly pale | Pale |