Overview
Three terms are commonly used when describing the types of fluid therapy:
- Resuscitation – given to patients in shock
- Replacement – given to correct fluid and/or electrolyte derangements and/or distribution problems
- Routine maintenance – given to maintain a patient’s normal fluid requirements
Normal fluid requirements
NICE state the following fluid requirements for maintenance fluids:
- 25-30 mL/kg/day of water and
- 1 mmol/kg/day of sodium, potassium, and chloride and
- 50-100 g/day of glucose to limit starvation ketosis
Potassium prescriptions based on weight should be rounded to the nearest common fluid available. Potassium should not manually be added as this is dangerous.
Prescribing Fluids: General Approaches
Overview
When prescribing fluids, first consider the patient:
- How old are they? – patients who are old and frail may be at risk of fluid overload
- How much does the patient weigh?
- What are their comorbidities? – e.g. heart failure can predispose to fluid overload
What is the prescription for?
The indications for prescribing fluids can broadly be categorised as:
What type of fluid will be given?
Crystalloids have a fixed amount of electrolytes (e.g. Hartmann’s has ~ 5mmol/L of K+).
0.9% saline and dextrose solutions can come with different mixed concentrations of K+ (usually 20 mmol or 40 mmol).
Potassium should never be manually added to a bag of fluids as this is dangerous. Further points regarding intravenous potassium administration are:
- The concentration of K+ should not exceed 40 mmol/L if given via a peripheral line as this can cause phlebitis and pain
- The rate should not exceed 10 mmol/hr. Rates above 20 mmol/hr require cardiac monitoring.
What rate is the fluid given at?
This depends on the indication. Some general rates are as follows:
- Resuscitation: a bolus (250-500 mL) over 15-30 minutes
- Maintenance fluids: 8-12 hourly
- Dehydration: 4-6 hourly
- Frail/elderly patients: 12 hourly with frequent assessment
Are additional electrolytes needed?
Electrolytes can be replaced orally or intravenously. Potassium is given as a pre-mixed solution with dextrose or sodium chloride. Other electrolytes may include:
- Calcium gluconate
- Magnesium sulphate
- Phosphate polyfusor
Review and reassessment
Continually reassess the response to fluids. Reassessment involves a clinical assessment (fluid balance), monitoring (such as urinary output or blood pressure), and laboratory testing (such as urea, creatinine, and electrolytes).
Definitions
Osmolality
Osmolality describes the number of particles per kilogram of liquid measured in milliosmoles per kilogram (mOsmol/kg). Osmolality does not change with temperature. A fixed amount of solid dissolved in a fixed mass of water will have the same osmolality at all temperatures.
Osmolarity
Osmolarity describes the number of particles per litre of liquid. This is measured in millimoles per litre (mmol/L). Since the volume of a liquid changes with temperature, osmolarity changes with temperature. If the temperature of a liquid increases, its volume increases as it expands. Therefore, osmolarity decreases with temperature. For this reason, osmolality is a preferred measurement in medicine.
Serum
Serum describes what is left in a blood sample once cells and clotting proteins are removed, leaving behind electrolytes, immunoglobulins, hormones, and exogenous substances.
Osmotic pressure
Osmotic pressure describes the pressure created when two solutions of different concentrations (water potentials) are separated by a semipermeable membrane that only allows water to pass through. The pressure is caused by the tendency of water to move from the side with a lower solute concentration (lower water potential) to the side with a higher solute concentration (higher water potential). The greater the difference in concentration between the two solutions, the greater the osmotic pressure.
Fluid Compartments and Fluid Shifts
Overview
The water in the body can be divided into conceptual compartments. These are not actual anatomic compartments but represent how fluid in the body is distributed. The main fluid compartments are the intracellular and extracellular compartments. Around 2/3 of the total water is held within cells in the intracellular fluid (ICF) space, and the rest is in the extracellular space.
Extracellular fluid can be subdivided into two main types:
- Interstitial compartment – intracellular fluid (fluid surrounding tissue cells)
- Intravascular compartment – inside the blood vessels and lymphatic vessels
When replacing fluids intravenously, these different compartments need to be accounted for. The type of fluid used and how it deposits in the correct compartment should be considered.
Fluid shifts
Fluids move between compartments by a combination of ultrafiltration (via a hydrostatic pressure gradient) and osmosis (via an osmotic pressure gradient). Water will continue to move passively until these gradients equalise.
When fluids move out of intravascular compartments, this can lead to hypotension and reduced perfusion of organs. When they move out of the intracellular compartment, cells become dehydrated, shrivel, and their cellular processes slow down.
When excess fluids accumulate in the intravascular compartment, oedema develops. When there are excess fluids in the intracellular compartment (which can happen due to too much fluid in the intravascular compartment), cells can become swollen and burst.
Third spacing
Third spacing describes the abnormal accumulation of fluid into the extracellular (outside of cells) and extravascular spaces (outside of blood vessels), leading to intravascular volume depletion and hypovolaemia. This causes hypotension and can lead to hypovolaemic shock.
Third spacing of fluid may occur in pancreatitis, sepsis, burns, intestinal obstruction, and post-operatively.
Types of Fluid
Tonicity
Fluids may be described as hypo-, iso-, or hypertonic compared to blood plasma:
- Hypotonic: has a lower concentration of dissolved solutes compared to plasma
- Isotonic: has a similar concentration of dissolved solutes to plasma:
- Hypertonic: has a higher concentration of dissolved solutes than plasma
Some fluids may be described as ‘balanced’. This means they have a similar electrolyte content to plasma. An example balanced crystalloid is Hartmann’s solution.
Hypotonic fluids
Hypotonic fluids describe fluids with a lower concentration of dissolved solutes compared to plasma. This causes fluids to shift from the extracellular fluid compartment into the intracellular fluid compartment.
Therefore, they are not useful for resuscitation as they do not stay in the intravascular compartment but are useful in replacing cellular fluid. They should be avoided in patients with increased intracranial pressure, as the movement of fluid into the intracellular compartment can cause cerebral oedema.
Examples are:
- 0.45% sodium chloride – good for replacing water in hypovolaemic patients with hypernatraemia. Excessive use can dilute sodium and cause hyponatraemia.
- Dextrose 5% (which is initially isotonic, but becomes hypotonic as the dextrose is metabolised)
Isotonic fluids
Isotonic fluids describe fluids with a roughly equal concentration of dissolved solutes as blood plasma. When administered, they expand both the intracellular and extracellular fluid compartments.
Therefore, they are useful for resuscitation and maintenance.
Examples are:
- 0.9% sodium chloride (normal saline):
- Ideal for expanding extracellular fluid compartment volume
- For each 1 L of 0.9% sodium chloride, around 1/3 remains in the intravascular compartment
- Used with caution in patients with heart failure, pulmonary oedema, and renal failure
- Using large volumes risks hyperchloraemic metabolic acidosis
- Dextrose 5% (which is initially isotonic, but becomes hypotonic as the dextrose is metabolised):
- When hypotonic, good for expanding the intracellular fluid compartment
- When isotonic, good for expanding the extracellular fluid compartment
- May be used for hypernatraemia as it provides water without sodium
- May be used in hypoglycaemia
- Should be avoided in patients with increased intracranial pressure as the expansion of the intracellular volume can cause cerebral oedema
- Hartmann’s solution:
- Contains electrolytes in quantities most similar to normal plasma and lactate, which is metabolised by the liver into bicarbonate
- Should be used with caution in patients susceptible to hyperkalaemia as it contains potassium
- Should be avoided where possible in patients with lactic acidosis or patients who cannot metabolise lactate (e.g. liver disease)
Hypertonic fluids
Hypertonic fluids describe fluids with a higher solute concentration compared to plasma. This causes the movement of water out of the interstitial and intracellular compartments into the intravascular compartment. This can lead to the shrinkage of cells and disrupt their function.
They can significantly affect electrolytes and are used with caution.
Examples are:
- 3% saline:
- May be used in treating severe hyponatraemia in critical situations under expert supervision. Drawing water into the intravascular compartment can ‘dilute’ the sodium in the plasma.
- May be used in cerebral oedema as drawing water out of the oedematous cells may be helpful.
Crystalloids and Colloids
Crystalloid solutions describe electrolytes and/or sugars that are dissolved in water. Common dissolved cations include sodium (Na+), potassium (K+), and calcium (Ca2+). Common anions include chloride (Cl–) and bicarbonate (HCO3–).
Commonly used crystalloids are as follows:
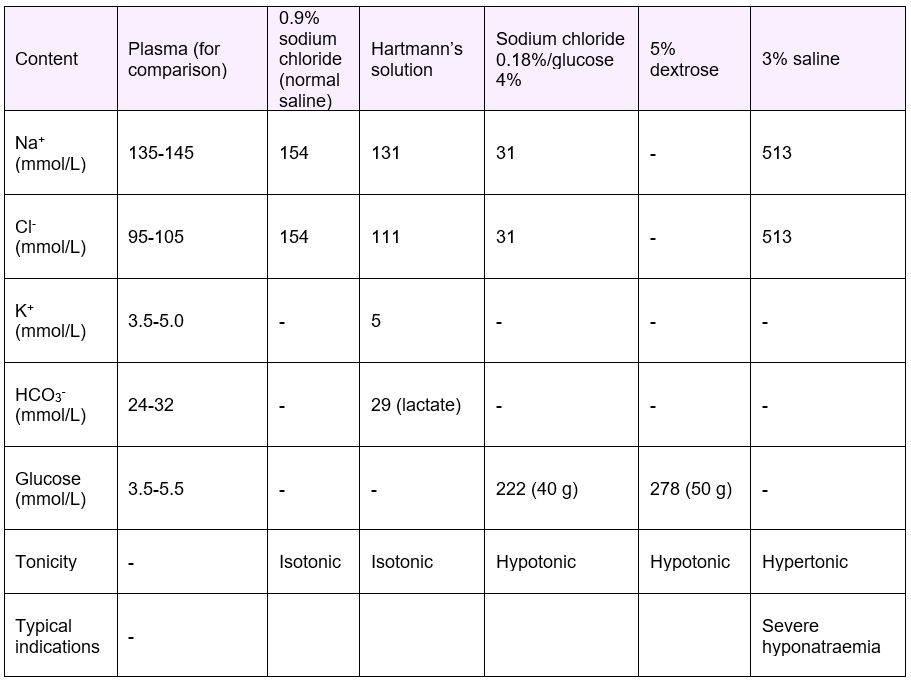
Colloids
Colloidal solutions contain starch or gelatin which exerts colloidal pressure (oncotic pressure) and electrolytes to maintain osmolality. The large starch or gelatin molecules do not pass through vascular membranes and stay in the intravascular compartment, holding water in the intravascular compartment and exerting osmotic pressure. This is normally done by albumin.
Colloids are less frequently used as they carry a risk of anaphylaxis. Furthermore, current evidence suggests that crystalloids are more effective in fluid resuscitation.
Resuscitation
Overview
Resuscitation IV fluids are given if the patient is in shock. Features suggesting the requirement for fluid resuscitation include:
- Systolic blood pressure <100 mmHg
- Heart rate >90 bpm
- Capillary refill >2 s or peripheries cold to the touch
- Respiratory rate 20 /min
- NEWS score ≥5
- Passive leg may predict fluid responsiveness
- This involves sitting the patient at 45 degrees and passively raising the legs to 45 degrees. An increase in pulse pressure and stroke volume suggests fluid responsiveness
Treatment
If fluid resuscitation is indicated. A bolus of fluid is given over 15-30 minutes:
- 500 mL is given to most people
- Smaller volumes (usually 250 mL) are given to people at risk of fluid overload (e.g. heart failure)
A crystalloid with a sodium content between 130-154 is generally used. Common crystalloids are 0.9% sodium chloride or Hartmann’s solution.
Reassessment
If the patient is still hypovolaemic, further fluid boluses can be attempted. Senior help should be sought if:
- There are signs of shock
- >2 L of fluid boluses have been given
Routine Maintenance
Overview
Routine IV fluids are given if the patient’s current oral intake is not sufficient to stay hydrated, for example, if a patient is ‘nil by mouth’. Before prescribing maintenance fluids it is important to determine the following:
- Does this patient require resuscitation?
- Do they have any complex fluid and/or electrolyte requirements?
- If so, see Replacement
Maintenance fluid requirements
NICE state the following fluid requirements for maintenance fluids:
- 25-30 mL/kg/day of water and
- 1 mmol/kg/day of sodium, potassium, and chloride and
- 50-100 g/day of glucose to limit starvation ketosis
Potassium prescriptions based on weight should be rounded to the nearest common fluid available. Potassium should not manually be added as this is dangerous.
Other considerations
For patients who are obese, adjust the IV fluid prescription to their ideal body weight and use the lower range of volume per kg (e.g. 25 mL/kg rather than 30 mL/kg) as patients rarely need more than 3 L of fluid per day.
Consider prescribing less fluid (e.g. 20-25 mL/kg/day) for patients who:
- Are older or frail
- Have renal impairment or cardiac failure
- Are malnourished and are at risk of refeeding syndrome
Replacement
Overview
Replacement IV fluids are given if the patient has an existing fluid deficit that cannot be corrected orally or it is impractical to do so (e.g. vomiting or increased insensible losses such as fever). All patients should be checked for if there are features of electrolyte disturbances, ongoing abnormal fluid or electrolyte losses, or issues with redistribution as these may need correction as well.
This requires continued evaluation and adjustment of maintenance fluids according to the following factors:
- Existing abnormalities:
- Some examples are dehydration, fluid overload, hyperkalaemia, or hypokalaemia
- Ongoing losses:
- Some examples are diarrhoea, blood loss, fever/sweating, pancreatic loss, fistula loss, urinary loss, vomiting, or nasogastric losses
- Redistribution and other complex issues:
- Some examples are gross oedema, severe sepsis, hypernatraemia or hyponatraemia, renal, liver, and/or cardiac impairment, post-operative fluid retention and redistribution, or malnourished and refeeding issues.
Treatment
Once the above factors have been taken into account, some changes may need making such as:
- Dehydration – more fluid may be required than the routine maintenance amount
- Fluid overload – less fluid may be required than the routine maintenance amount
- Hyperkalaemia or hypokalaemia – less or more potassium may be required
These estimates should be added or subtracted from the routine maintenance amount worked out from the routine maintenance section above.