Overview
Diabetes insipidus (DI) is characterised by increased thirst and the production of large amounts of dilute urine as a result of inadequate antidiuretic hormone (ADH, also known as vasopressin) function. DI can be associated with hypernatraemia.
There are 4 forms of DI:
- Cranial DI:
- Decreased secretion of ADH
- Nephrogenic DI:
- Kidneys do not respond to ADH effectively
- Gestational DI:
- Only during pregnancy, the placenta produces an enzyme called vasopressinase that breaks down ADH
- Dipsogenic DI (primary polydipsia):
- Due to increased intake of fluids without impaired ADH function
- This can be due to damage to thirst mechanisms in the hypothalamus or psychiatric illness
To help make sense of this chapter, it may be helpful to refer to Endocrine and Metabolic Physiology.
Risk Factors
Cranial DI
- Idiopathic
- Head trauma/surgery
- Pituitary tumours
- Pituitary surgery
- Craniopharyngioma
- Sarcoidosis
- Haemochromatosis
- Meningitis/encephalitis – usually seen in late disease
- Subarachnoid haemorrhage
Nephrogenic DI
- Genetic mutations:
- Most are mutations in the ADH receptor
- Others can be mutations coding for aquaporin 2 channels
- Drugs:
- Lithium
- Demeclocycline
- Gentamicin
- Rifampicin
- Other:
Presentation
The presentation of DI can be vague and insidious. Features are:
- Polyuria
- Polydipsia
- Nocturia
- Signs of hypernatraemia:
- Irritability
- Lethargy
- Spasticity
- Hyperreflexia
Differential Diagnoses
Psychogenic polydipsia
- Patients may have an underlying psychiatric condition
- Waking at night with the need to drink water rather than pass urine is more suggestive of primary polydipsia
- Water deprivation tests are normal
Diabetes mellitus
- Although signs and symptoms may be similar, blood glucose is elevated
Hypercalcaemia
- Blood shows hypercalcaemia
- Bones – bone pain and fractures
- Stones – renal stones
- Abdominal groans – anorexia, nausea
- Psychiatric moans – depression, insomnia, impaired memory
- Thrones – constipation
- An ECG may show QT interval shortening
Investigations
- U&Es and calcium:
- Sodium: may be normal/elevated
- An elevated sodium + low urine osmolality is strongly suggestive of DI
- Potassium: may be normal or low in nephrogenic DI
- Calcium: may be normal or high in nephrogenic DI
- Serum glucose:
- Normal – done to exclude diabetes mellitus
- Serum osmolality:
- Normal or elevated
- Urine osmolality:
- Reduced (<300 mOsm/kg)
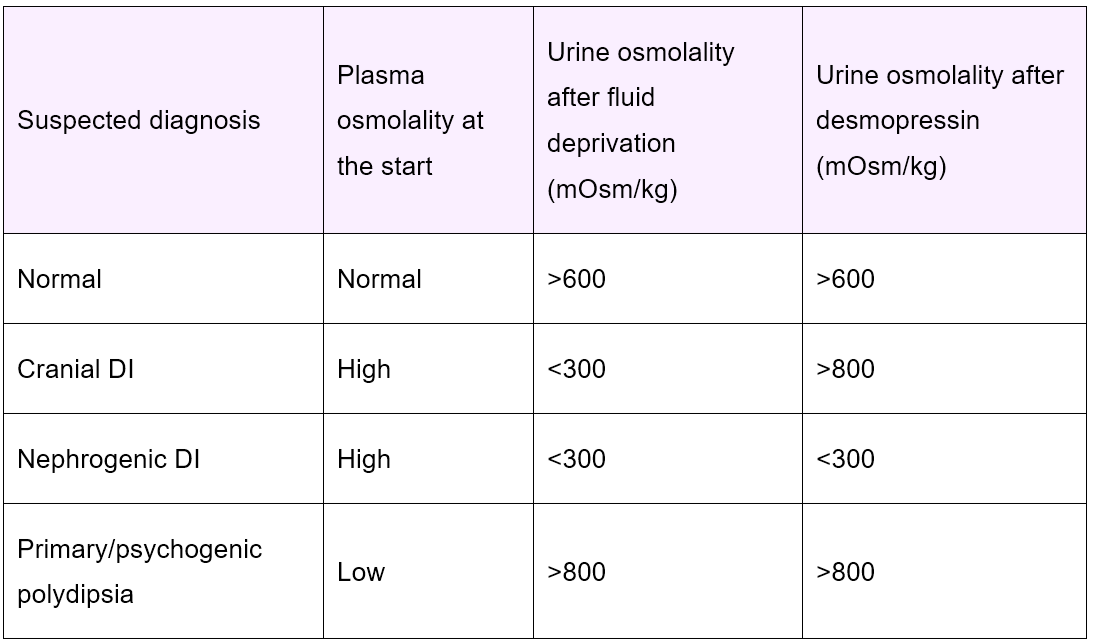
- Water deprivation test:
- Patients have their urine osmolality, are deprived of fluids for 8 hours, and then have it measured again
- See interpretation of results below
- Desmopressin stimulation test:
- Patients are given desmopressin and the urine osmolality is measured.
- See interpretation of results below
Management
- Cranial DI: desmopressin
- Nephrogenic DI: thiazide diuretics, high-dose desmopressin, and NSAIDs may be considered
Complications
- Hypernatraemia:
- Can occur if patients do not drink water while feeling thirsty due to DI
- Iatrogenic hyponatraemia:
- Replacement desmopressin can lead to hyponatraemia
- Bladder dysfunction and/or hydronephrosis:
- In cases of nephrogenic DI
Prognosis
- Mortality is rare as long as water is available
- Once treatment and correct fluid management has been put in place, the prognosis is usually very good