Overview
Glaucoma describes the damage to the optic nerve with progressive loss of retinal ganglion cells and their axons. It is usually due to a raised intraocular pressure (IOP), however many patients have an IOP within the normal range, or many have a raised IOP with no development of glaucoma.
Primary open-angle glaucoma is a chronic progressive optic neuropathy in the absence of other ocular diseases or related conditions.
Ocular hypertension is where there is a consistently elevated IOP (usually >21mmHg) with no signs of glaucoma.
Pathophysiology
Normally, intraocular pressure is maintained by the flow of aqueous humour. The ciliary body secretes fluid into the posterior chamber, which flows to the iris and through the pupil into the anterior chamber. The fluid then leaves through the trabecular meshwork or uveoscleral outflow routes. The angle is the part of the eye where the iris meets the cornea and sclera and the trabecular meshwork is found here.
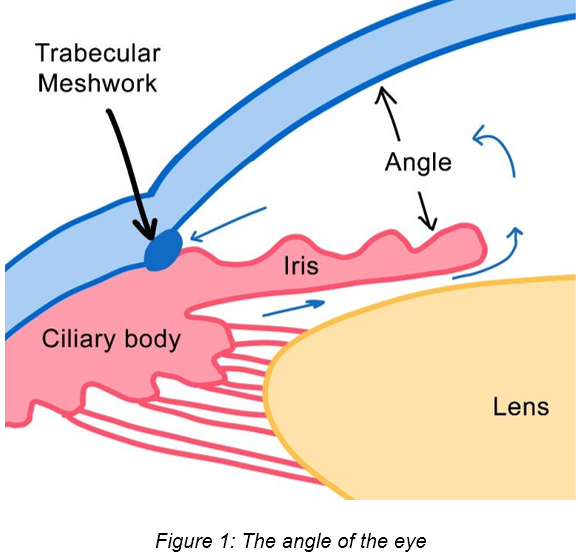
Primary open-angle glaucoma is thought to be due to a progressive increase in resistance through the trabecular meshwork, making it more difficult for aqueous humour to flow through and leave the eye. This leads to a chronic increase in intraocular pressure, giving rise to glaucoma.
Epidemiology
- Primary open-angle glaucoma is the most common form of glaucoma
- Prevalence increases with age
- Globally, primary open-angle glaucoma is the second leading cause of blindness
Risk Factors
- Raised intraocular pressure
- Myopia
- Increasing age
- Family history
- Black ethnicity
- Corticosteroid use
- Type 2 diabetes mellitus
- Cardiovascular disease
- Hypertension
Presentation
Signs and symptoms come on very insidiously and many patients are asymptomatic until severe visual loss and permanent damage have occurred. This is usually because vision loss happens in the peripheries. Patients may have:
- Vision loss affects the periphery moving inwards, leading to “tunnel vision”
- Decreased visual acuity
Fundoscopy Findings
- Optic disc cupping (normal range is 0.4-0.7)
- Optic nerve cup notching
- Optic disc pallor – this suggests optic nerve atrophy
Differential Diagnoses
Acute angle closure glaucoma
- Pain is present, along with features of systemic upset (e.g. nausea/vomiting)
- Eye redness may be present
- Hazy cornea may be present
- Halos may be seen
- Dark rooms may worsen the pain as it causes mydriasis
Ocular hypertension
- Raised intraocular pressure without any signs or symptoms of optic nerve damage
- Visual fields are normal
Screening
Some populations are entitled to free NHS-funded eye examinations by optometrists:
- Family history of glaucoma
- Aged 60 or over
- People who have been advised by an ophthalmologist that they are at risk of developing glaucoma
Investigations
- Fundoscopy:
- May show:
- Optic disc cupping
- Optic nerve cup notching
- Optic disc pallor
- May show:
- Tonometry:
- May show elevated intraocular pressure
- Slit-lamp examination – assesses cornea, anterior chamber, and the angle
- The cornea is usually clear
- The angle should be open
- Gonioscopy – assesses the anterior chamber between the cornea and iris and assesses fluid drainage
- The angle is not obstructed
Management
- 1st-line: prostaglandin analogue eyedrop
- Options are: latanoprost, travoprost, or tafluprost
- 2nd line: beta-blockers or carbonic anhydrase inhibitors or alpha-2 adrenergic agonist eyedrops or combination treatment
- Beta-blocker options are: timolol or betaxolol
- Carbonic anhydrase inhibitor options are: dorzolamide or brinzolamide
- Alpha-2 adrenergic agonist options: brimonidine or apraclonidine
- 3rd line: cholinergic eyedrops (e.g. pilocarpine)
- Consider surgery (e.g. trabeculectomy) or laser treatment in advanced cases
Drugs used in Glaucoma
Prostaglandin analogues
- Mechanism of action:
- Increases uveoscleral outflow and drainage of aqueous humour
- Adverse effects:
- Increased brown pigmentation of the affected eye
- Lengthening of the eyelashes
- Dry eyes
- Contraindications:
- Pregnancy
- Breastfeeding
- Acute uveitis
Beta-blockers
- Mechanism of action:
- Reduces aqueous secretion by the ciliary body by inhibiting beta-adrenoceptors
- Adverse effects:
- Irritation
- Dry eyes
- Conjunctivitis
- Contraindications:
- Bradycardia
- Heart block
- Asthma
- COPD
- Untreated heart failure
Carbonic anhydrase inhibitors
- Mechanism of action:
- Reduces aqueous secretion by the ciliary body
- Adverse effects:
- Discomfort
- Lacrimation
- Keratitis
- Uveitis
- Contraindications:
- Renal impairment
- Severe hepatic impairment
- Allergy
- Breastfeeding
Alpha-2 adrenergic drugs
- Mechanism of action:
- Reduces aqueous secretion and increases outflow through the trabecular meshwork
- Adverse effects:
- Mydriasis
- Dry eyes
- Eye redness
- Contraindications:
- Acute angle-closure glaucoma due to mydriatic effects
- Patients taking monoamine oxidase inhibitors
Cholinergic drugs
- Mechanism of action:
- Causes ciliary muscle contraction which opens up drainage channels in the trabecular meshwork
- Adverse effects:
- Miosis – can cause blurred vision
- Headaches
- Contraindications:
- Uveitis
Monitoring
- Patients both with primary open-angle glaucoma and ocular hypertension should be followed up regularly, usually every 3-12 months. The frequency of follow-up depends on the degree of disease.
Patient Advice
- Patients should be taught how to administer eyedrops effectively and should take them as prescribed. They should not stop taking their eyedrops without seeking advice.
- Patients should seek help if they notice any changes in vision, redness, or pain.
Complications
- Irreversible vision loss
Prognosis
- As primary open-angle glaucoma progresses insidiously, patients are often asymptomatic until late in the disease
- Any vision lost due to glaucoma cannot be restored