Overview
Parkinson’s disease (PD) is a chronic and progressive extrapyramidal neurological disorder due to the degeneration of dopaminergic neurones in the substantia nigra. This leads to the classical features that can be remembered using the acronym “TRAP”:
- Tremor
- Rigidity
- Akinesia/bradykinesia
- Postural instability
Parkinsonism describes the features and symptoms associated with Parkinson’s disease. Drug-induced Parkinsonism can happen with the use of drugs that block dopamine receptors or reduce the amount of dopamine available.
It may be helpful to read about Extrapyramidal Symptoms for the following chapters.
Parkinson-plus syndromes
Parkinson-plus syndromes are conditions characterised by features of Parkinson’s disease (tremors, rigidity, akinesia/bradykinesia, and postural instability) but also include additional features such as dementia, cognitive impairment, and cranial nerve impairment. These can include:
Epidemiology
- Parkinson’s disease is the second most common neurodegenerative disorder following Alzheimer’s disease
- Typically develops between 55-65 years
- Men are affected more than women
Causes of Parkinsonism
- Parkinson’s disease (idiopathic Parkinson’s)
- Vascular Parkinsonism
- Due to restricted blood supply to the brain
- Can develop following a stroke
- Chronic head trauma
- Drug-induced Parkinsonism:
- Antipsychotics
- Metoclopramide
- Domperidone does not cross the blood-brain barrier and therefore does not cause extrapyramidal side effects
- Multiple system atrophy
- Progressive supranuclear palsy
- Normal pressure hydrocephalus
- Wilson’s disease
Risk Factors
- Increasing age
- Family history
- Chronic exposure to pesticides
- Male sex
- Head trauma
Presentation
Overview
The onset of Parkinson’s disease is insidious. Parkinson’s disease symptoms are usually unilateral. The classical features can be remembered with the acronym “TRAP”:
- Tremor:
- A 4-6Hz “pill-rolling” tremor is seen at rest
- Improves with the use of the affected limb
- Rigidity:
- Cogwheeling, especially if a tremor is present
- Limbs are often described as a “lead pipe”
- Posture may be stooped
- Akinesia/bradykinesia:
- Slowness in movement
- Short and shuffling steps
- Reduced arm swing in gait
- Difficulty initiating movement
- Postural instability:
- Imbalance or falling
- Particularly when turning
- In drug-induced Parkinsonism, the symptoms are usually bilateral and more rapid in onset.
Other features seen in Parkinson’s disease may be:
- Depression
- Common in people with Parkinson’s disease
- Masked facies
- Reduced animation of the face and expression
- Hypokinetic dysarthria
- Reduced pitch variation – speech is monotone
- Hypophonia – quieter voice
- Fatigue
- REM sleep dysfunction
- Autonomic dysfunction:
- Constipation
- Postural hypotension
- Parkinson’s dementia
Atypical features
Features of atypical Parkinsonism may suggest another condition such as multiple system atrophy, or suggest drug-induced Parkinsonism:
- Acute onset of symptoms
- Rapidly progressive disease
- Cognitive impairment
- Severe autonomic dysfunction
- Neuropsychiatric features such as hallucinations, fluctuating consciousness
Differential Diagnoses
Drug-induced Parkinsonism
- History of precipitating drug may be present: antipsychotics/metoclopramide/lithium
- Symptoms may be bilateral
Progressive supranuclear palsy
- Postural instability and falls early in the disease
- Gaze palsies – looking down affected more than looking up
- Poor response to levodopa
Multiple system atrophy
- Autonomic dysfunction prominent:
- Erectile dysfunction
- Urinary/faecal retention or incontinence
- Postural hypotension
- Speech or bulbar dysfunction
- Cerebellar dysfunction
- Poor response to levodopa
Essential tremor
- Progressive tremor in upper extremities
- Tremor usually disappears on rest and worsens with use
Dementia with Lewy bodies
- Dementia that precedes Parkinson’s disease
- Hallucinations
- Fluctuating mental status
Normal pressure hydrocephalus
- Acute/subacute onset
- Dementia
- Incontinence
- Gait abnormalities
Investigations and Diagnosis
Overview
Parkinson’s disease is only diagnosed and managed by a specialist with expertise in movement disorders.
- Any patient with suspected Parkinson’s disease should be urgently referred to a specialist.
- Specialists may trial a dopaminergic agent and this can help confirm the diagnosis.
Other investigations
If atypical Parkinsonism is suspected, or another pathology is suspected, the following may be ordered:
- MRI brain
- SPECT
- Serum caeruloplasmin and copper studies
- For Wilson’s disease
Management
Overview
There is no cure. Treatment is symptomatic and aims to supplement depleted dopamine stores. Treatment is tailored to the patient’s individual lifestyle circumstances, preferences, needs, and goals.
In general:
- If motor symptoms impact quality of life: levodopa
- If motor symptoms do not impact quality of life: levodopa or dopamine agonists or monoamine oxidase B (MAO-B) inhibitors.
- NICE does not recommend giving ergot-derived dopamine agonists first-line
NICE has produced the following table comparing different Parkinson’s medications. This can be used to help guide decisions regarding initiating treatment:

Adverse effects of drugs used in Parkinson’s disease may be:
- Excessive sleepiness
- Hallucinations
- Impulsivity e.g. gambling, hypersexuality, inhibition etc. – these are more likely with:
- Dopamine agonist therapy
- A history of previous impulsive behaviours
- A history of alcohol consumption and/or smoking
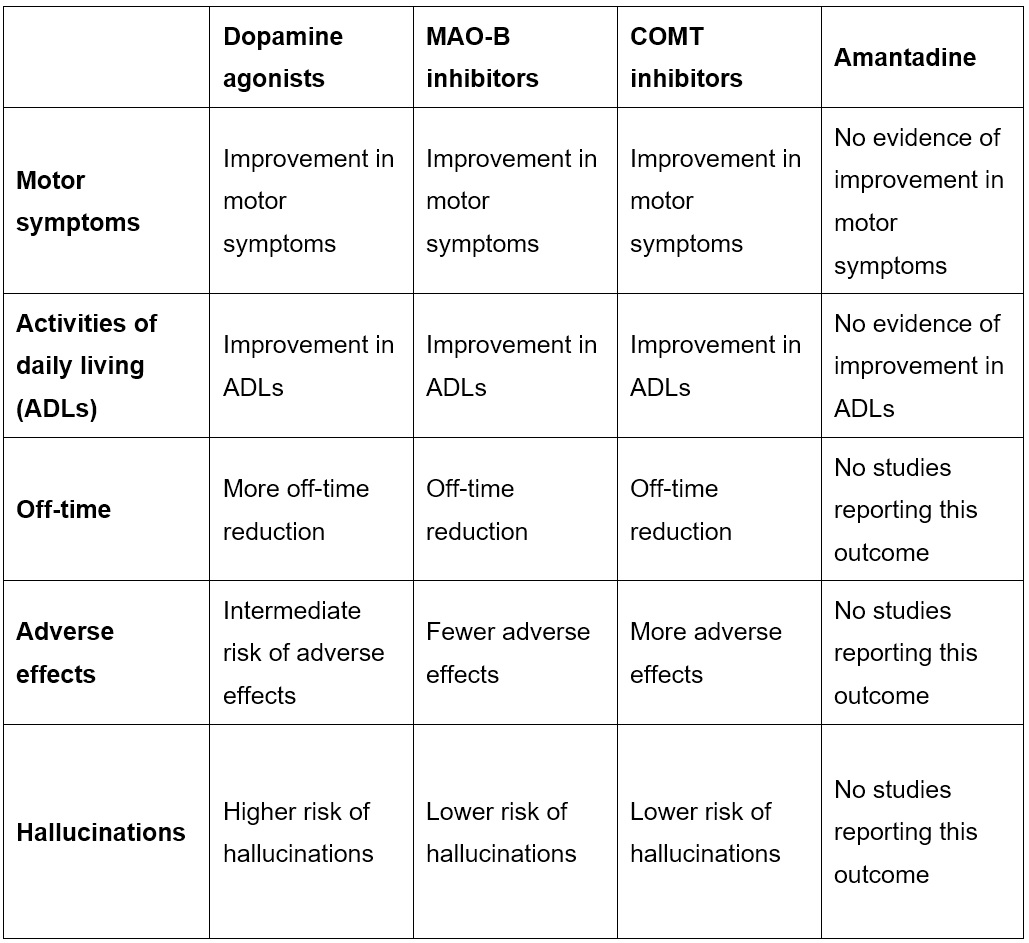
If patients have developed motor symptoms such as dyskinesia or motor fluctuations, NICE recommends adding one of the following to levodopa therapy:
- Dopamine agonists
- MAO-B inhibitors
- Catechol-O-methyltransferase (COMT) inhibitors
NICE has produced the following table comparing different adjuvant Parkinson’s medications. This can be used to help decide which drug to add to levodopa therapy.
Management of complications
Management of other associated complications are:
- Excessive daytime sleepiness:
- Patients should not drive
- Changes to medication regimes
- Modafinil if medication changes do not help
- Orthostatic hypotension:
- Review medications and identify possible causative medications
- Midodrine can be considered
- Drooling of saliva:
- Consider glycopyrronium
- Parkinson’s dementia:
- Rivastigmine
On-off periods
Pharmacological management of Parkinson’s disease can lead to an improvement in symptoms known as the “on-period”. Some patients have worsening symptoms, known as the “off-period”. These periods are related to the amount of levodopa in the blood.
Off-periods can suggest that the medication is wearing off. “Motor fluctuations” describes the effect of having less control of motor symptoms after a period of having them well-controlled.
In the early stages of Parkinson’s disease, patients may not notice when levodopa is wearing off, but as it progresses, they find that a dose does not last as long as it originally did, leading to more fluctuation between on- and off-periods.
Drugs used in Parkinson’s Disease
Overview
Some key points include:
- Diagnosis and treatment are initiated by a specialist in movement disorders
- Any changes to medication are carried out by a specialist in movement disorders or at least has input from a specialist
- Parkinson’s drugs should never be withdrawn abruptly or stopped
- This may cause acute akinesia or neuroleptic malignant syndrome
- “Drug holidays” are not advised to reduce motor symptoms
- This may cause acute akinesia or neuroleptic malignant syndrome
- Any patient admitted to hospital with Parkinson’s disease must have their medicines given at the exact times needed
- A delay may risk acute akinesia or neuroleptic malignant syndrome
- If a patient cannot take levodopa orally, they can be given a dopamine agonist patch
- Antipsychotics may worsen Parkinson’s disease
- Clozapine may be a good option for psychosis in Parkinson’s disease
Levodopa
Usually combined with peripheral dopa-decarboxylase inhibitors – an example is co-beneldopa (benserazide and levodopa)
- Adverse effects:
- On-off effect is seen
- Acute dystonia may happen if abruptly stopped
- Dyskinesia
- Dry mouth
- Anorexia
- Postural hypotension
- Psychosis
- Impulsive behaviours e.g. gambling/spending/inappropriate sexual behaviour
Dopamine receptor agonists
Less effective than levodopa
Examples are:
- Non-ergot-derived: ropinirole/pramipexole/apomorphine
- Ergot-derived: bromocriptine/cabergoline
- Adverse effects similar to levodopa but more common and severe
- Ergot-derived options should only be used if non-ergot-derived dopamine agonists fail to work
- This is because they are associated with pulmonary fibrosis
Monoamine oxidase-B (MAO-B) inhibitors
Examples are selegiline and rasagiline
Adverse effects are:
- Postural hypotension
- Arrhythmia e.g. atrial fibrillation
- Hypertension if taken with tyramine-rich foods e.g. mature cheese, salami, marmite etc.
Catechol-O-methyltransferase inhibitors
Examples are entacapone and tolcapone
Amantadine
Mechanism is not fully understood. Thought to be a weak dopamine agonist.
Adverse effects are:
Patient Advice
- Regarding medication:
- Patients should take medications as instructed
- Levodopa should be taken 1-2 hours before eating food to maximise its effectiveness
- Patients may need to make lifestyle changes:
- If there is postural instability, avoid activities needing good balance
- Patients should consider stopping driving if symptoms are severe or cognitive deficits are present
- Regular exercise is beneficial
- A symptom diary can help treat complications
Complications
- Dyskinesia secondary to levodopa
- Motor fluctuations – “on-off periods”
- Parkinson’s dementia
- Autonomic dysfunction – constipation/orthostatic hypotension
- Psychosis
- Depression and anxiety
- Disinhibition and impulsivity
- Daytime sleepiness
Prognosis
- Parkinson’s disease is slowly progressive and has no cure
- Severity varies significantly