Overview
Iron deficiency anaemia describes reduced haemoglobin due to low iron stores in the body. It is the most common cause of anaemia globally and is more common in children and young women.
Iron is essential for haemoglobin synthesis and red blood cell (RBC) production. The body normally replenishes iron through recycling iron from old RBCs and dietary absorption.
It is not a diagnosis itself and requires further investigation for underlying causes. New IDA in an adult without a clear underlying cause may suggest the presence of gastrointestinal tract cancer.
It may be helpful to look at the chapter on Anaemia: Data Interpretation alongside reading this section to help wrap your head around when to suspect what type of anaemia.
Epidemiology
- IDA is the most common cause of anaemia globally
- IDA is more common in young children
- IDA is more common in premenopausal women due to menorrhagia and pregnancy
Causes
Iron losses
- GI tract losses (e.g. colorectal cancer) are the most common cause in men and post-menopausal women
- Menorrhagia is the most common cause in pre-menopausal women
- Aspirin/NSAID use
- Colorectal cancer, gastric cancer
Dietary causes
- Dietary insufficiency is more common in growing children and the elderly
- Dietary insufficiency alone is a rare cause – it takes around 8 years for an adult male to develop IDA due to a poor diet
Malabsorption
- Gastric surgery
- Coeliac disease
- Inflammatory bowel disease
- Helicobacter pylori
Increased requirements
- Pregnancy
- Growing children
- Erythroderma
Risk Factors
- Menorrhagia
- Pregnancy – due to increased demand
- Strict diets e.g. vegetarian/vegan
- Chronic kidney disease
- Coeliac disease
- Gastric surgery
- NSAID use – due to increased risk of peptic and duodenal ulcers
- Chronic heart failure
Presentation
Iron deficiency anaemia is often picked up incidentally instead of being the main presenting complaint. general features of anaemia are:
- Fatigue
- Shortness of breath, particularly on exertion
- Palpitations and tachycardia
- Impaired growth in children
- Pallor
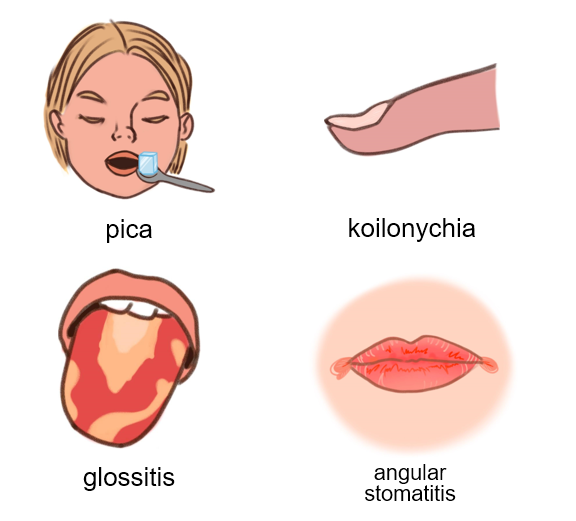
Features that suggest iron deficiency are:
- Hair loss
- Brittle nails or koilonychia (spoon-shaped nails)
- Atrophic glossitis
- Angular stomatitis
- Pica – abnormal craving for items that are not food e.g. paint, ice
- Restless legs syndrome (RLS) – there is an association between IDA and RLS
Differential Diagnoses
Anaemia of chronic disease
- Total iron-binding capacity (TIBC) is usually low
- This is because ferritin decreases in inflammation, leading to fewer binding ‘spots’ for iron to bind to, resulting in a low TIBC
- Ferritin is usually normal/high
- Ferritin is a positive acute-phase reactant
Investigations
All patients
- Full blood count:
- Haemoglobin: low
- Platelets: usually normal but can be deranged
- Mean cell volume:
- Low
- Other red cell tests:
- Mean corpuscular haemoglobin (MCH): low
- Mean corpuscular haemoglobin concentration (MCHC): low
- Red cell distribution width (RDW): increased
- Blood film:
- Small, pale (hypochromic) red cells with:
- Anisocytosis (variation in size) and
- Poikilocytosis (variation in shape) – some may be ‘pencil’-shaped
- Small, pale (hypochromic) red cells with:
- Reticulocyte count:
- May be low (bone marrow does not have enough iron to make RBCs)
- Iron studies:
- Serum iron:
- Decreased
- Total iron-binding capacity (TIBC):
- Increased
- This is increased because there are more open binding sites for iron to attach to due to the deficiency in iron
- Serum ferritin:
- Decreased
- Transferrin saturation:
- Decreased
- This is because fewer binding sites are taken up by iron due to its deficiency
- Serum iron:
- Coeliac serology:
- Coeliac disease may be an underlying cause:
- IgA and anti-TTG, EMA antibodies are tested
- Endoscopy:
- Considered in men and post-menopausal women with IDA and no obvious cause
- Consider H.pylori testing if recurrent IDA and normal upper and lower endoscopy findings
Example blood tests
| Haemoglobin: | 104 g/L | (130 – 180 g/L) |
| Platelets: | 205 x 109/L | (150 – 450 x 109/L) |
| Mean cell volume (MCV): | 67.5 fL | (76.0 – 98.0 fL) |
| White blood cells: | 8.5 x 109/L | (3.00 – 10.0 x 109/L) |
| Serum iron: | 10.3 μmol/L | (11.6 – 35.0 μmol/L) |
| Serum ferritin: | 15 ng/mL | (25 – 350 ng/mL) |
| Total iron-binding capacity (TIBC): | 96 μmol/L | (45 – 81 μmol/L) |
Cancer and Referral
Overview
IDA in an individual without a clear underlying cause (e.g. heavy menstruation) may suggest the presence of malignancy, such as gastrointestinal tract cancer. Postmenopausal bleeding may cause IDA in postmenopausal women, which may suggest endometrial cancer.
NICE recommends:
- Referring the following patients with IDA using a suspected cancer pathway referral (within 2 weeks):
- ≥60 years
- <50 years and have rectal bleeding
- Referring the following patients to gastroenterology:
- All men and postmenopausal women with IDA unless it is obvious that the cause is non-gastrointestinal (GI)
- All people ≥50 years even if coeliac disease is found
- Premenopausal women who have colonic symptoms, a strong family history of GI cancer, persistent IDA, or do not menstruate (e.g. hysterectomy)
- Referring the following patients to gynaecology:
- Menorrhagia does not respond to medical treatment
- Post-menopausal bleeding via suspected cancer pathway referral
- Pregnant and significant symptoms/severe anaemia, late gestation, or failure to respond to oral iron
Management
All patients
- 1st-line: manage underlying cause and refer if necessary
- Oral iron replacement for 3 months e.g. ferrous sulfate
- If not tolerated: IV iron replacement
Monitoring
- Recheck haemoglobin via full blood count within the first 4 weeks – should rise by 20g/L over 3-4 weeks:
- Refer if there is a lack of response (<20g/L rise) after 2-4 weeks
- If full blood count findings return to normal, continue iron treatment for 3 months then stop:
- After this, monitor the FBC periodically, usually every 3 months for 12 months then every 6 months for 2-3 years
- If haemoglobin drops again, prescribe iron replacements again
- Consider referral if haemoglobin cannot be maintained via replacement or there is evidence of underlying pathology e.g. weight loss, chronic unexplained diarrhoea, persistently increased inflammatory markers or persistent/recurring IDA
Patient Advice
- Iron-rich foods may be of use:
- Examples are dark green vegetables, meat, iron-fortified bread
- Advise patients about avoiding accidental overdose and keeping iron supplements out of sight of children. An overdose can be fatal.
- Patients are likely to get adverse gastrointestinal effects, particularly constipation. This can be minimised by taking iron supplements with or after food and usually settles down with time.
Complications
- Developmental delays in children
- Impaired muscle performance
- High-output heart failure:
- Where the heart is pumping normal/higher amounts of blood out to the body but this is still insufficient, causing strain
- Increased infection risk
- Complications in pregnancy e.g. low birthweight and preterm delivery
Prognosis
- The prognosis depends on the underlying cause.